Brain tumors
Brain tumors comprise a large group of varied lesions that manifest in different ways. Treatment goals and recommendations are therefore very diverse and tumor-specific.
First, a diagnosis is sought. Sometimes magnetic resonance imaging (MRI) is sufficient to give a confident diagnosis, but it is usually necessary to take tissue samples at the time of surgery. This may be done through a biopsy or by performing a resection of the tumor. Recently there has been some significant progress in the genetic analysis of tumor samples, in addition to the standard “microscopic” appearance to help make treatment decisions. This is particularly true for “gliomas” and other “primary” tumors.
The two broad categories of brain tumors are primary tumors (arising from brain tissue) and secondary tumors (starting outside the brain and traveling or compressing the brain). Some brain tumors are biologically benign. These tumors do not need postoperative treatments unless there is recurrence or a potentially aggressive pathology. Many primary tumors and the vast majority of secondary tumors will require additional postoperative treatment: either radiation therapy, chemotherapy or both.
The benefits of an initial tumor resection include: diagnostic accuracy, relief of direct and indirect pressure effects, potential cure and, in many cases, improvement in overall outcome by assisting adjuvant postoperative treatments. Surgical planning and recommendations are of course highly individualized and depend on a variety of factors. Clinical and radiologic evaluation will help determine the risk and benefits and, therefore, the appropriateness of surgery.
Glioma
This is a very broad term that describes a group of tumors originating from “glial” or supporting cells of the brain. These tumors range from low grade and slow growing to high grade and fast growing. The treatment depends on the type and grade of the tumor, as well as on a number of clinical factors. Tissue sampling or biopsy is necessary to establish the diagnosis. Various subtypes include astrocytoma, GBM (glioblastoma multiforme), oligodendroglioma, ependymoma, medulloblastoma, neurocytoma and ganglioglioma.
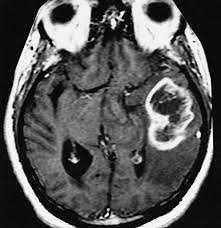
A Glioma that causes compression effects and “edema” (swelling).
GBM (Glioblastoma Multiforme)
This is the most common type of a primary brain tumor and nearly always requires surgery. Given that the tumor is intrinsic and that it grows around nerve fibers, it is usually not possible to cure it. Instead, most of the accessible tumor will be safely removed. After the operation, radiation therapy and chemotherapy are administered. Genetic testing of the tumor is also very helpful in determining the best treatment.
Low-grade gliomas
A low-grade glioma is usually a slow-growing lesion with a characteristic appearance on MRI and CT scans. Treatment remains controversial and varies from observation only to biopsy or resection (removing the tumor).
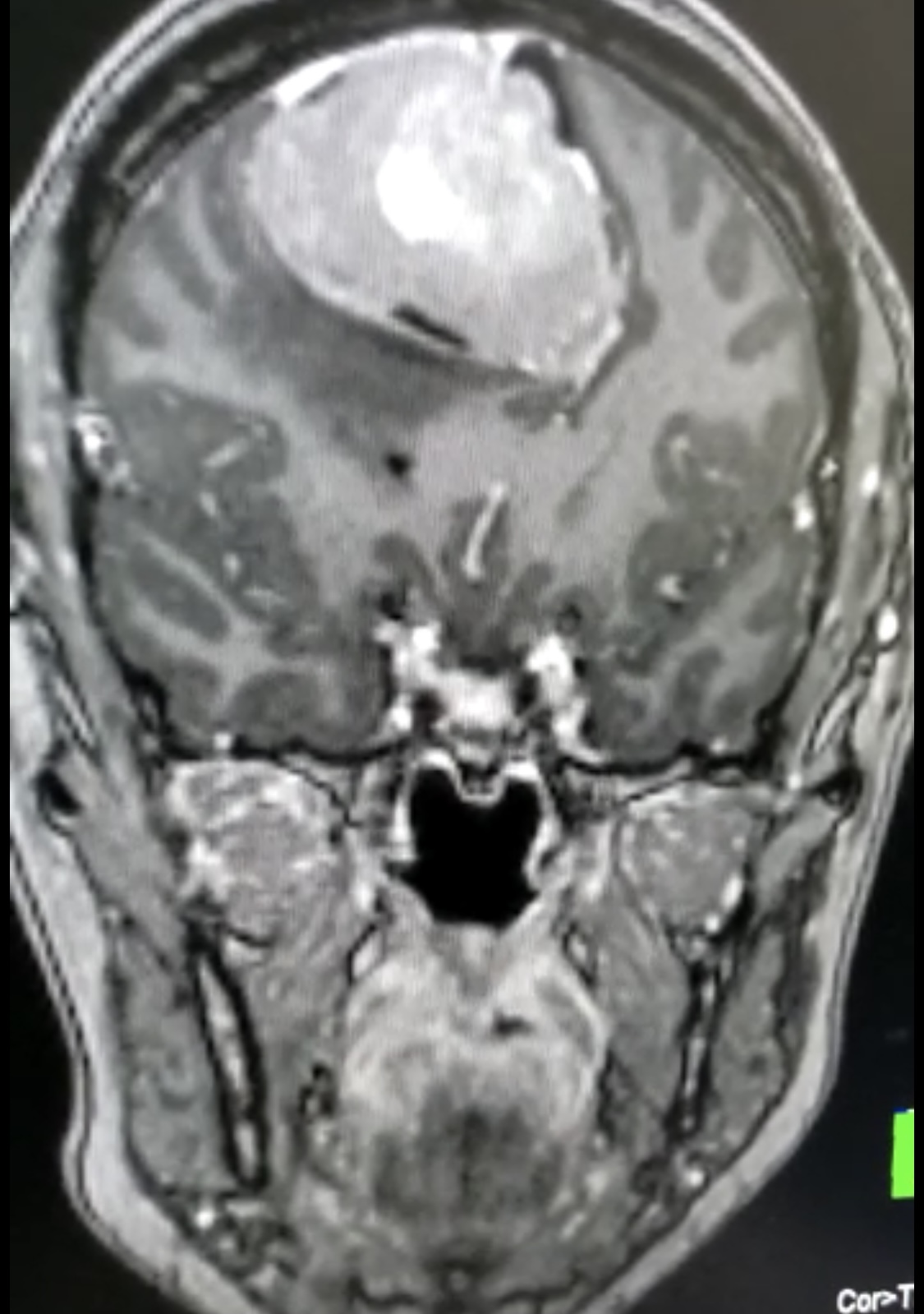
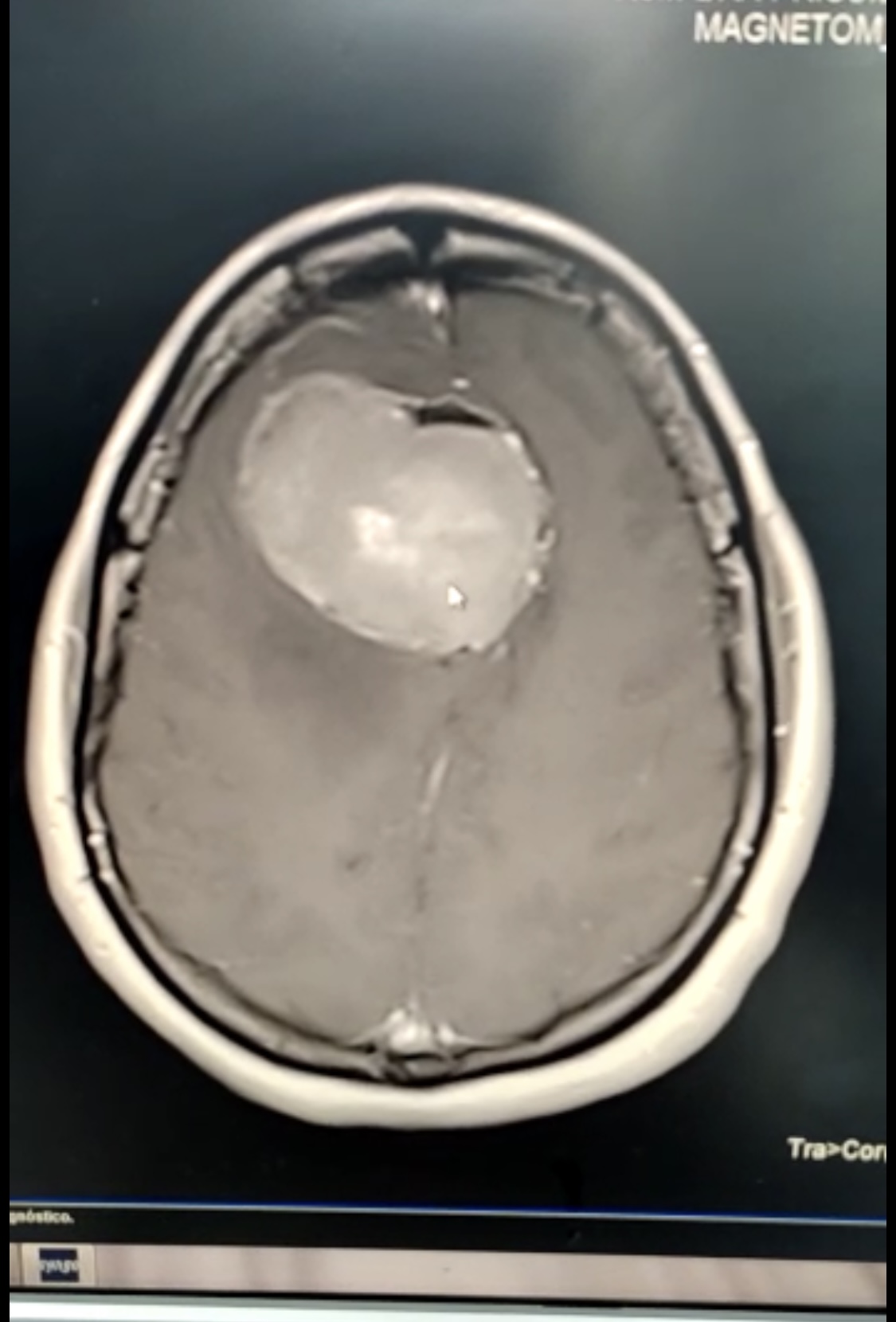
Meningioma
These tumors start outside the brain and usually compress it slowly. They have a very characteristic appearance on MRI and CT scans. Surgery is recommended when there is tumor growth on serial imaging, tumor-related symptoms or uncertainty with the diagnosis. Surgery is usually quite simple in this case, depending on accessibility, and patients are often effectively cured. However, long-term MRI surveillance is recommended.
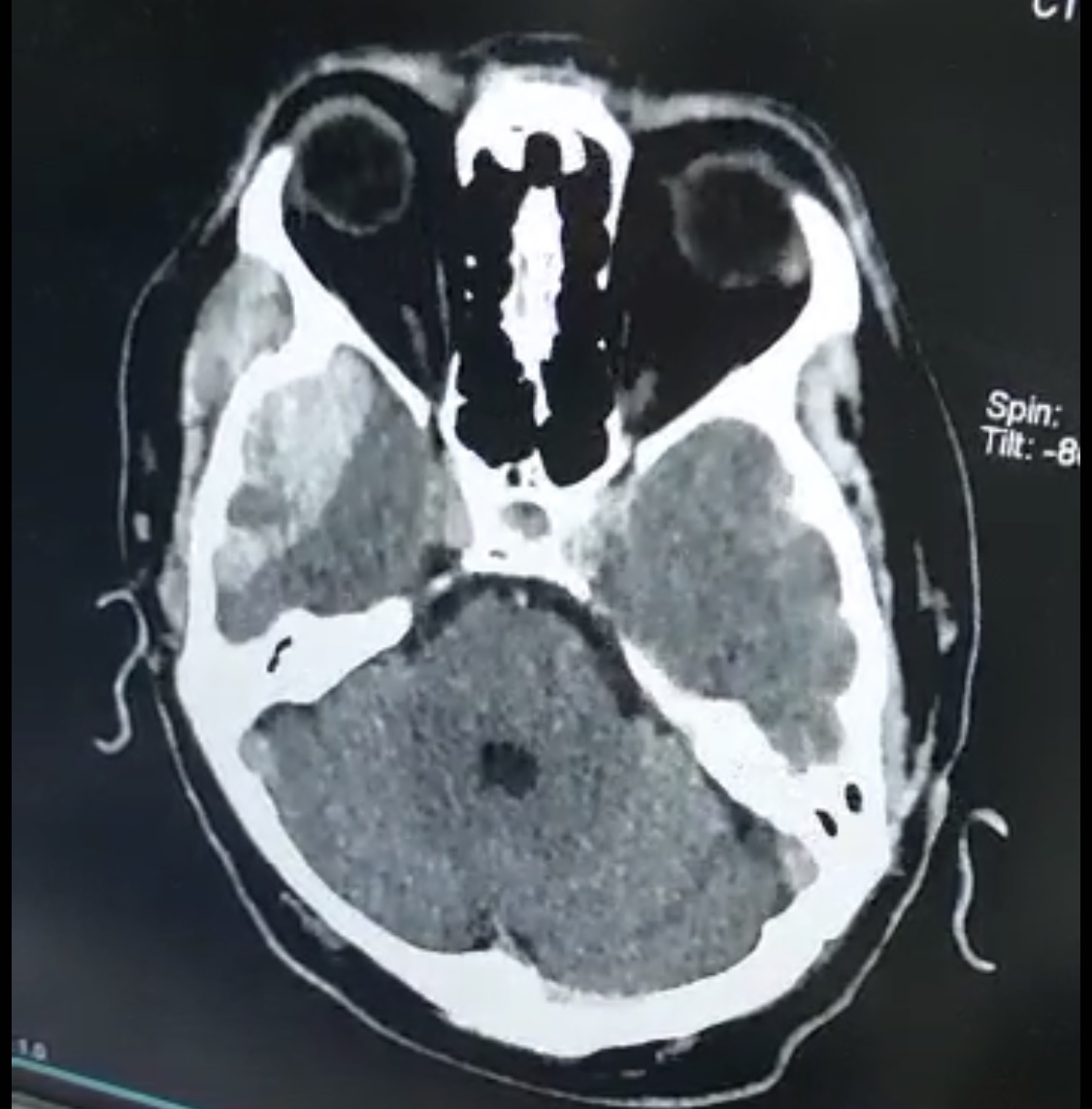
Acoustic neuroma (Schwannoma)
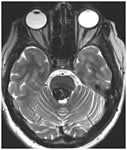
This special type of tumor has a higher degree of complexity and may occur as part of an inherited syndrome. The tumor arises from the balance and hearing nerve and therefore patients often experience hearing loss. This tumor is also closely related to nearby cranial nerves and can cause compression and dysfunction of the underlying brainstem. Treatment decisions depend on a myriad of factors, but range from periodic observation and monitoring, surgical resection or volume reduction, or treatment with stereotactic radiation (radiosurgery).
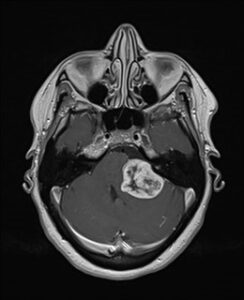
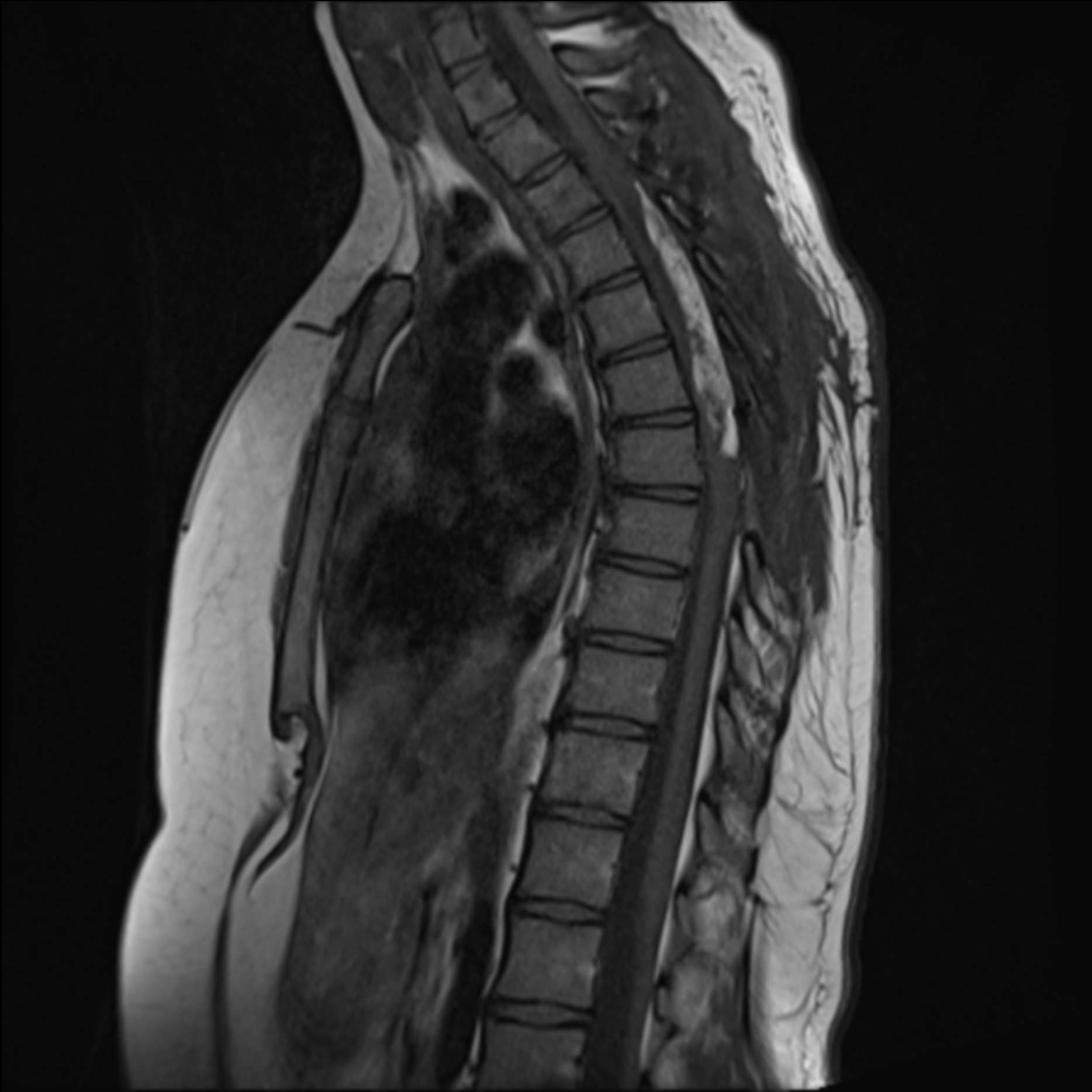
A large acoustic neuroma with brainstem compression.
Metastatic cancer
When a primary tumor spreads from its place of origin, it is usually transported by the bloodstream. The brain is an important site for secondary deposits and these tumors have a very characteristic appearance on MRI. They often cause substantial brain swelling. If the primary site is unknown or if one or more lesions are symptomatic and accessible, surgical removal is usually recommended.
Pituitary tumors
Pituitary tumors are a specific group of lesions that are located below the visual apparatus (optic nerves) at the base of the skull. When there is sufficient enlargement, these tumors can cause visual disturbances by compressing the optic nerves or chiasm from below. They also often present hormonal imbalances called endocrinopathy, either because of too much or too little of a specific hormone. Due to their location in the midline immediately behind the nose, they are easily accessible with minimally invasive approaches in case of a surgical intervention. In other words, they can be surgically removed through the nostrils.
Hydrocephalus
Hydrocephalus refers to a problem with the normal circulation of “CSF” (cerebrospinal fluid) through the deep chambers or ventricles of the brain and around the special fluid spaces around the brain. It leads to a buildup of intracranial fluid and/or pressure, which can cause a number of neurological problems, such as headaches, trouble walking and difficulty with cognitive performance (thinking and memory). In its acute forms it can be imminently life-threatening. Occasionally, the cause is a blockage within the fluid chambers, blocking from the inside, but more often, no discrete blockage is seen and the problem is to be found in the spaces surrounding the brain or in fluid absorption. The most common way to treat this problem is with a “ventriculoperitoneal shunt”, but in some cases a “third ventriculostomy” (minimally invasive endoscopic procedure) will effectively prevent acute hydrocephalus.

Ventriculoperitoneal shunt placed for “hydrocephalus”.
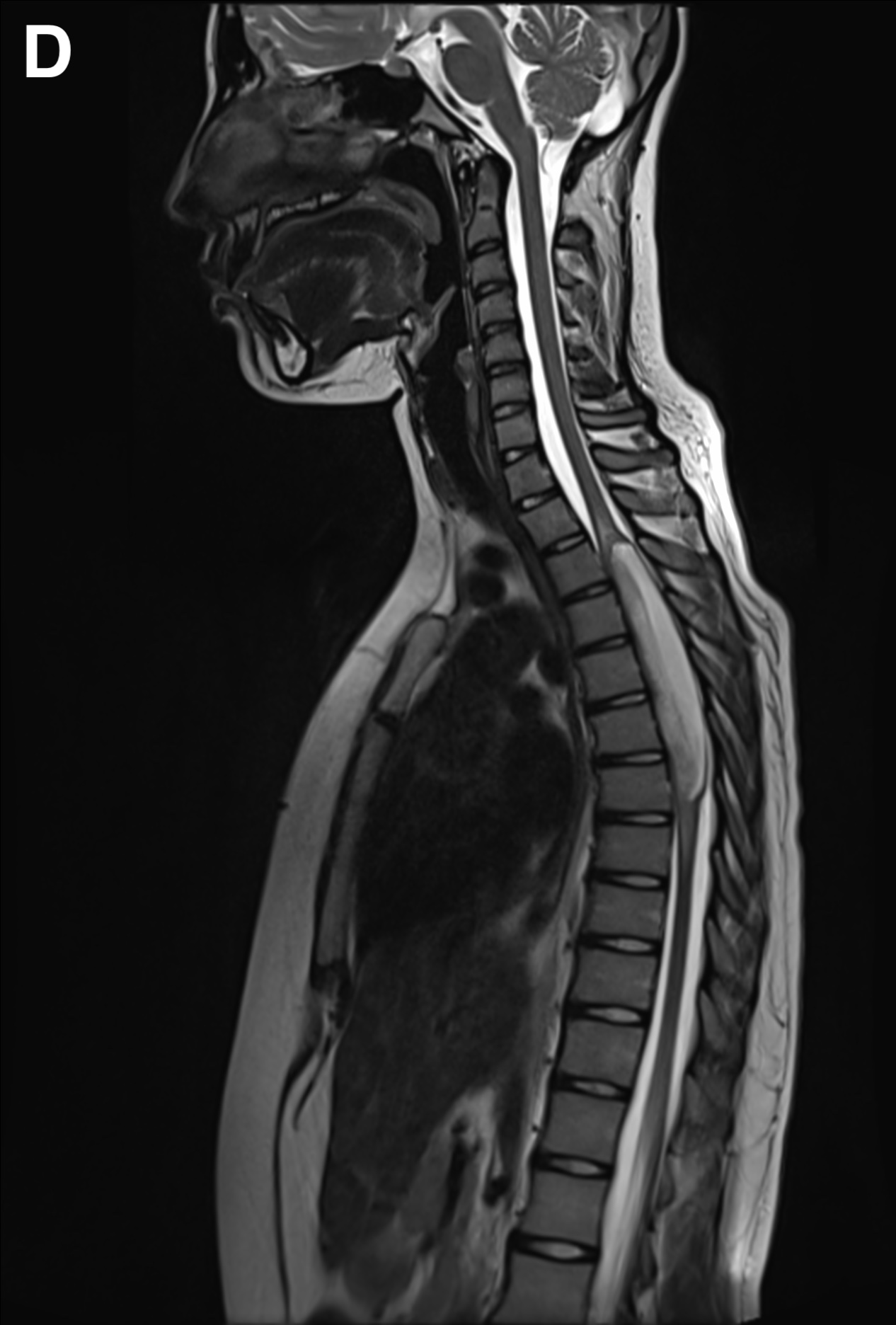
Chiari Malformation
Chiari malformations comprise a group of developmental disorders that result in an abnormal position of the “hindbrain”. The most common type is a type 1 lesion, where part of the balance structure called the cerebellum is positioned too low. This leads to compression of the underlying brainstem and secondary problems with fluid accumulation. When symptomatic or when there are obvious pressure problems, surgical intervention is recommended. The goal of surgery is to create enough space at the site of the obstruction to relieve compression and prevent further fluid pressure buildup.
Trauma
Trauma can result in a wide range of neurosurgical problems. Occasionally, the trauma is so trivial that there is no memory of the actual event. The most common problem needing treatment is a “subdural hematoma” and “epidural hematoma”. Surgery is recommended if there are pressure effects on the brain or symptoms of compression. The recommended intervention ranges from a simple trepanation hole (trephination) to removal of the clot through a major craniotomy/craniectomy (removal of a part of the skull).
Aneurysms
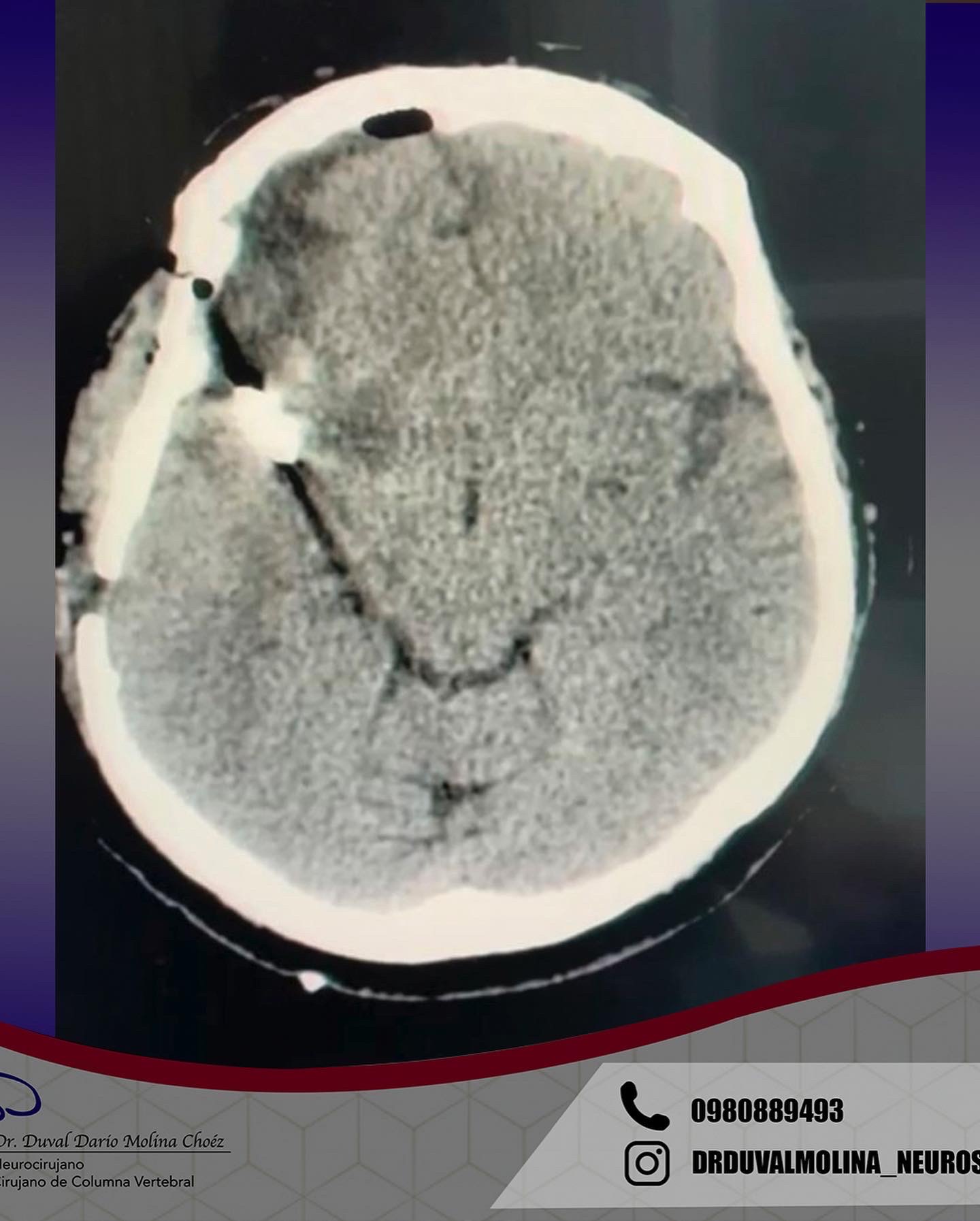
Aneurysms are bulges in an arterial wall that represent weak points. They are found in about 2-3% of the population and usually remain undetected until they rupture. A ruptured aneurysm leads to a very severe headache and a rapid onset of neurological problems. The characteristic pattern of hemorrhage is called a “subarachnoid hemorrhage.”
Aneurysms can also cause instant death or result in permanent disability. In some cases, there is a strong family history or genetic condition. The most common inherited disorder is adult polycystic kidney disease. Trigger factors for aneurysm rupture include smoking, poorly controlled hypertension, and overexertion. If left untreated, there is a cumulative annual risk of rupture and periodic screening is recommended.
The typical bleeding pattern is seen after aneurysm rupture. The shape and location of the aneurysm can predict its behavior and also determine which treatment is preferred. Alternatively, if the aneurysm has a low risk of rupture or a high surgical risk, we may choose to surveil it with serial imaging. The intervention is designed to block the blood flow into the aneurysm, therefore eliminating the risk of hemorrhage. It can be performed endovascularly – by filling the aneurysm from within (“endovascular coiling”), or by open microsurgical techniques (“clipping”).

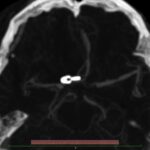
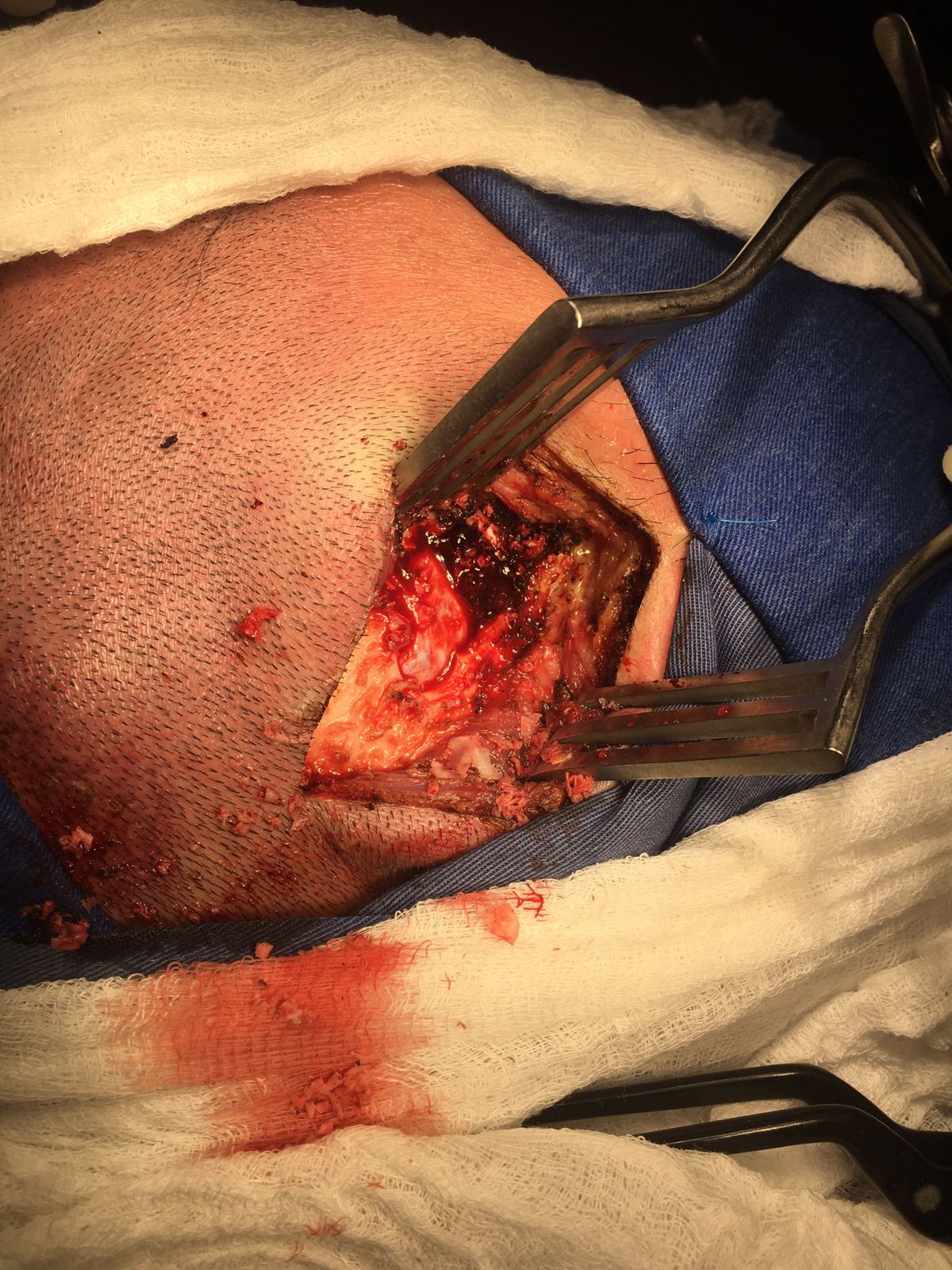
Surgical clipping (resolution)
A small incision is made behind the hairline and a piece of bone is removed to allow access to the aneurysm. The aneurysm is identified under microsurgical vision, with its branches and one or more clips applied externally to its neck. When the aneurysm is healed, the bone is replaced with special titanium plates and the incision is closed.
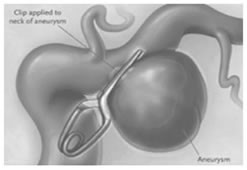
Clipped aneurysm

Aneurysm clip and support
- Arteriovenous malformations (AVMs)
Arteriovenous malformations or AVMs are congenital anomalies that affect the blood vessels in a specific region of the brain. They result from a disruption of the normal, progressive sequence of blood vessel wall type from artery to capillary to vein. Instead of this sequential change, there is a nidus or tangle of vessels under arterial pressure, which diverts blood directly from the high-pressure arterial circulation to the venous circulation, with no slowing down and little decrease in pressure. The result is constant high flows and elevated pressure throughout the AVM. This generates abnormal vessel shear stress and can lead to vessel wall rupture and spontaneous hemorrhage.
In addition to the local consequences of high flow and elevated venous pressures, the nearby brain is deprived of its blood flow. This is particularly true with large AVMs and can result in what is known as the “steal” syndrome. This can cause neurological problems, if the nearby brain is functionally important or “eloquent”. AVMs can manifest in spontaneous hemorrhage, seizures, a neurological problem or deficit, or headaches. With CT and MRI being much more prevalent these days, they can also be found incidentally.
Treatment decisions are based on balancing the estimated risk of immediate and future bleeding (“cumulative lifetime risk”) versus the risk of eradicating the lesion with treatment. Clearly, despite the use of complex tables and statistical methods, it is not possible to know with certainty the natural history of any individual. It is stated that the annual risk of hemorrhage associated with an AVM lies between 2 and 4%. There are certain risk factors that may increase this likelihood, such as a previous hemorrhage, arterial or intranidal aneurysms, restricted venous flow, and underlying respiratory or medical conditions. Each hemorrhage also entails the possibility of death or stroke and disability.
Several imaging modalities can be used to define the AVM. Computed Tomography (CT) and its variant Angiotomography provide information on the location and static vascular anatomy, including the vessels supplying and draining the AVM. Magnetic resonance not only tells us where in the brain the AVM is located, it also helps to measure risk and surgical approaches and provides information on previous hemorrhages. Cerebral angiography provides detailed dynamic information on flow patterns and venous drainage. Although it is the most sensitive and powerful test, it is also technically more “invasive” and entails a very small risk of stroke.
Treatment recommendations can range from observation and medication to microsurgical excision, but other forms of treatment are becoming more prominent worldwide. The internal blocking of the arterial feeders, through the artery, is called “embolization” and is extremely helpful in making the surgery safer. It is usually a preoperative maneuver. Occasionally, it may be the only treatment required.
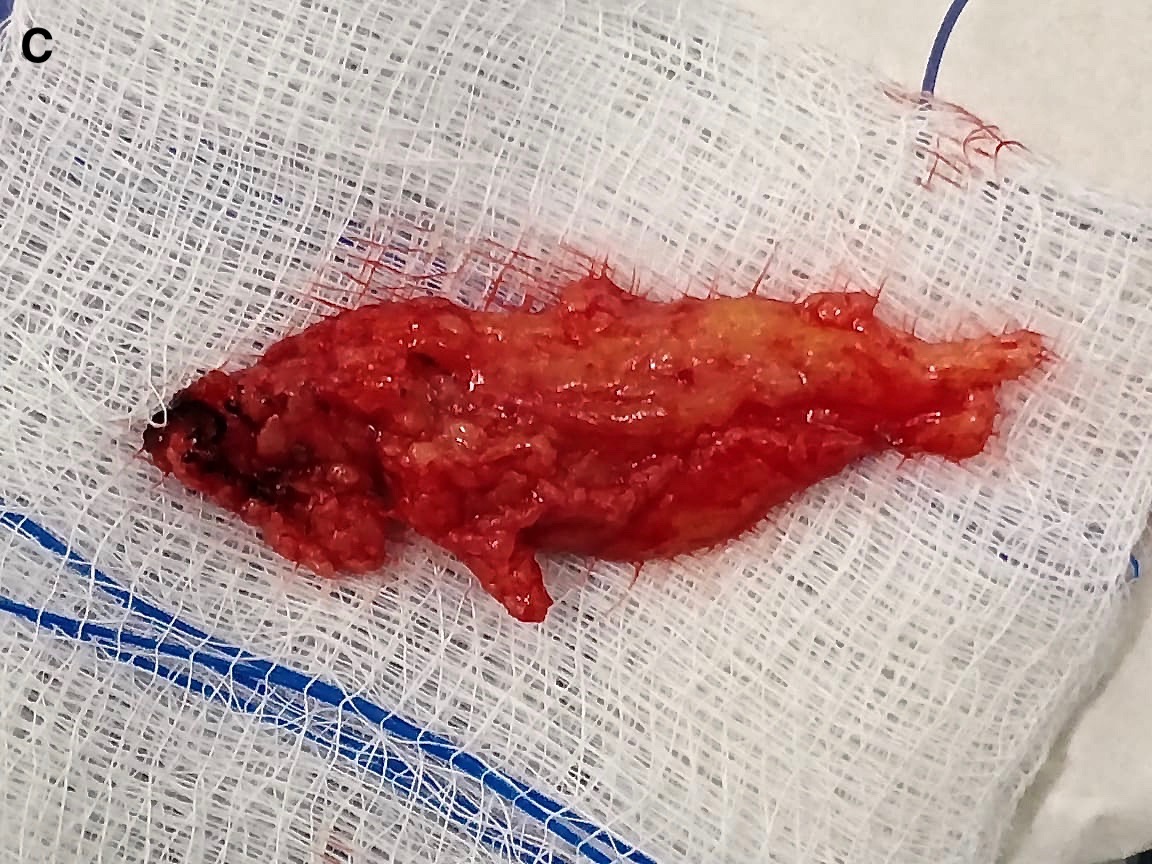
Malformation
Post-resection
Arteriovenous malformations can also be cured with “radiosurgery”. This procedure involves the use of powerful computers to direct an array of radiation beams into the AVM volume. AVM shapes are often complex and a great deal of planning is needed in targeting them. This form of treatment does not have an immediate effect and results in slow obliteration of flow within the AVM over several years. Of the low-volume lesions that are treated, 70 to 85% will heal. MRI and progress angiograms are needed to establish a cure. Lesions of 3 cm used to be the upper limit in size for targeted lesions, but it is possible to treat larger lesions if the “marginal” dose – the dose that is directed towards the edge of the lesion – is reduced. A correct marginal dose is needed to obtain the best balance between lesion healing and brain protection.
Radiosurgery planning

Linac Stereotactic Radiosurgery
Cavernous malformations
Cavernous malformations are focal collections of thin-walled widened vessels under low pressure and low flow. There is usually evidence of previous hemorrhage in or around the lesion and they have a very characteristic magnetic resonance (MR) appearance. Familial forms occur and may be solitary or multiple. They may manifest in seizures, neurologic events or hemorrhage or may be discovered incidentally. The lesions that do not cause symptoms are observed with MRI. Accessible symptomatic malformations are eliminated.
A cavernous malformation of the brainstem.
Moyamoya disease
Little is known about Moyamoya; a disease of the main arteries at the base of the brain. In response to the progressive narrowing seen in the large arteries, a network of thin vessels forms in an attempt to maintain blood supply to the starved brain. The condition shows Transient Ischemic Attacks (TIA) or ischemia, or intracerebral hemorrhage. Cerebral angiography can provide a definitive diagnosis. Treatment consists of a variety of strategies from observation to extracranial-intracranial bypass surgery. Endovascular treatments are not usually recommended because of vessel fragility and restenosis. In addition, some relatively simple procedures can improve blood flow and help with symptoms.
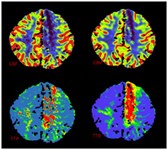
Typical CT perfusion findings in someone with Moya Moya’s disease

Recurrent aneurysm seen near clips
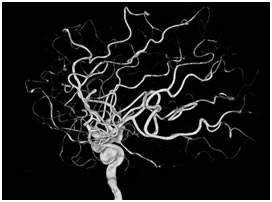
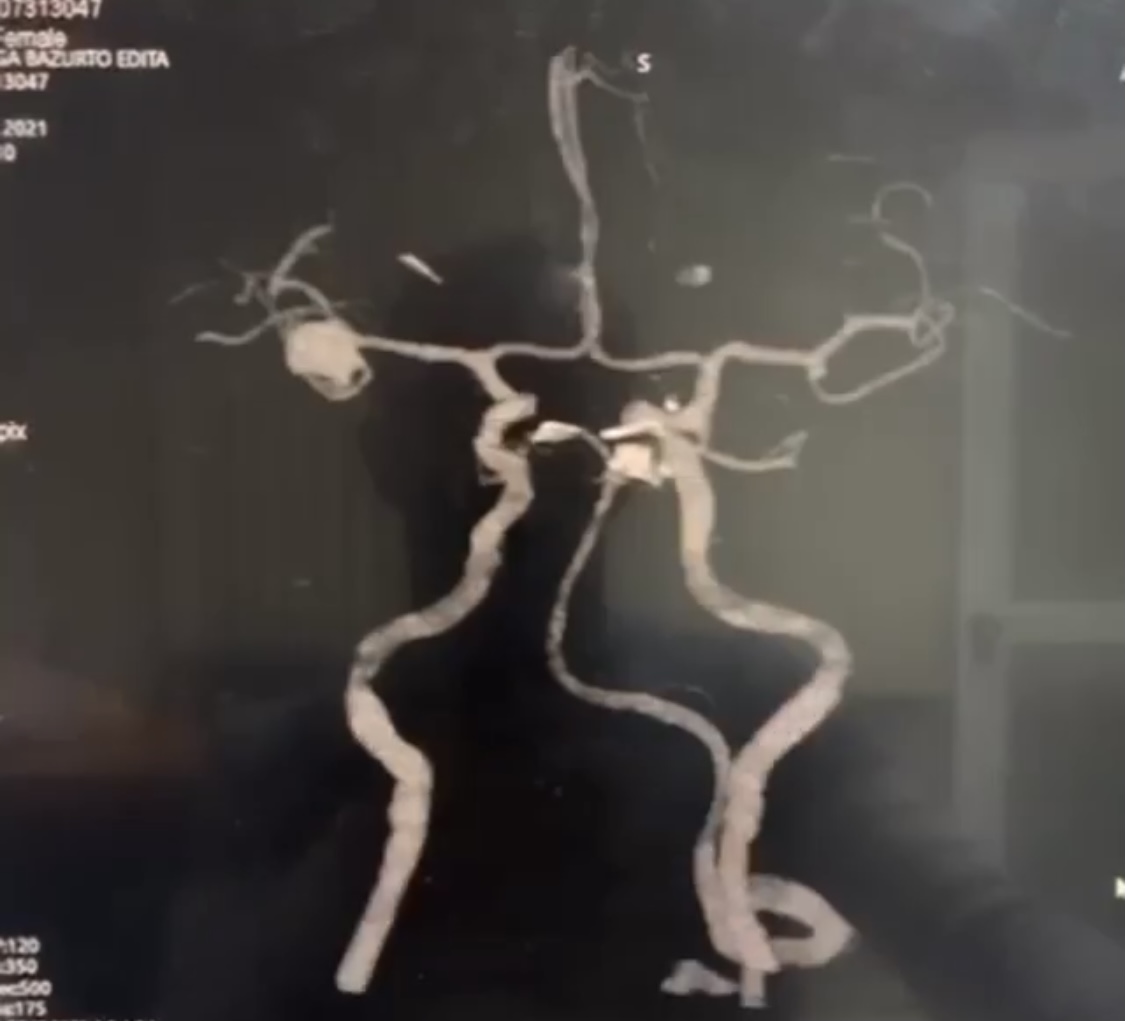
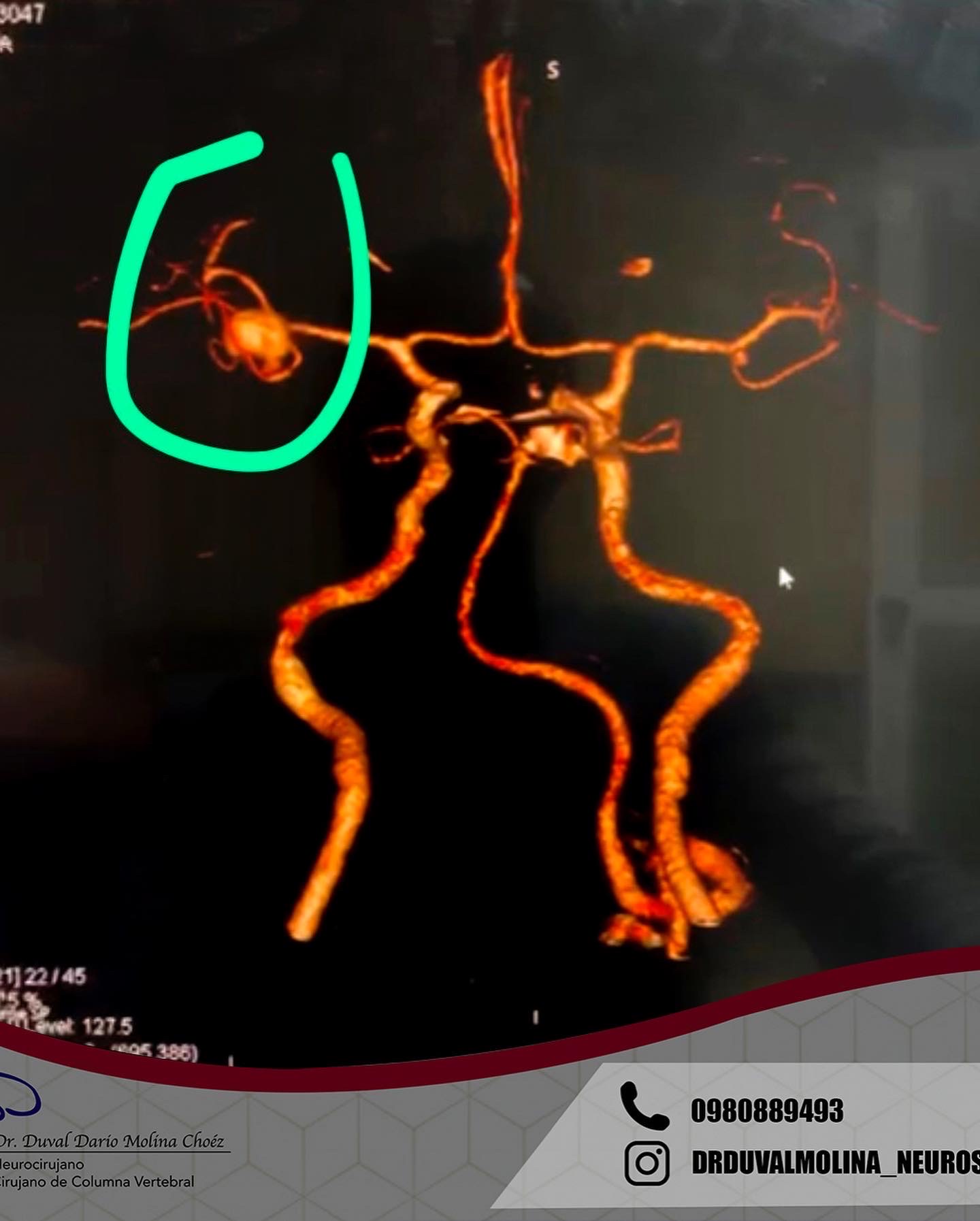
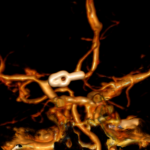
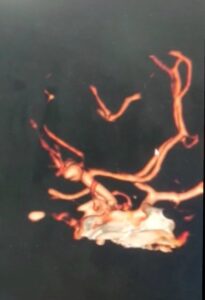
3D brain angiography showing an aneurysm